RASS
The Richmond Agitation Sedation Scale (Figure) is an arousal scale that has been traditionally used to monitor depth of sedation and underlying brain dysfunction in the intensive care unit (Sessler et al. Am J Respir Crit Care Med. 2002 and Ely et al. JAMA. 2003). However, its role has expanded beyond the intensive care unit. The RASS is part of several delirium assessments. The RASS has been evaluated as a standalone delirium assessment. Unlike the CAM, bCAM, CAM-ICU 3D-CAM, and 4AT, which requires the rater to perform cognitive testing on the patient, the RASS simply requires the rater to observe the patient during routine clinical care.
In older emergency department patients, an abnormal RASS is 82% to 84% sensitive and 85% to 88% specific for delirium when performed by physicians and non-physicians (Han et al. Acad Emerg Med. 2015, LINK PENDING). Tieges et al. investigated the mRASS in older post-operative hip fracture patients and found a RASS other than 0 to be 80% sensitive and 90% specific for delirium (Tieges et al. Am J Geriatr Psychiatry. 2013). Chester et al. investigated the modified RASS (mRASS), which is a RASS with an informal test of inattention, in older medical inpatients. They observed that a mRASS other than 0 was 64% sensitive and 93% specific for delirium (Chester et al. J Hosp Med. 2012). However, Marcantonio et al. found that only 18% of older medical patients with delirium had altered level of consciousness (Marcantonio et al. Ann Int Med. 2014).
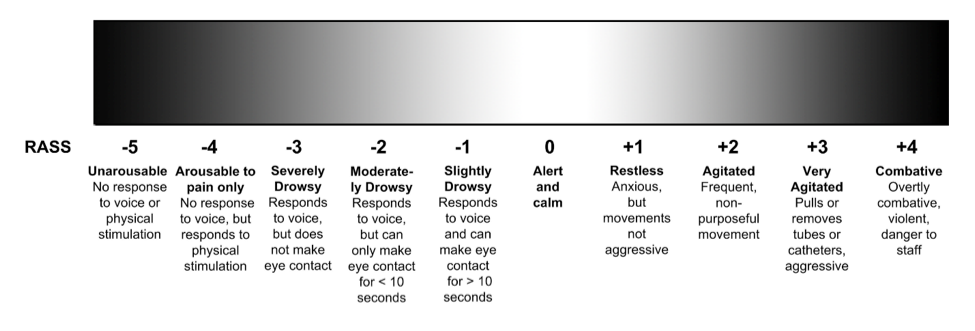
Figure. Richmond Agitation Sedation Scale (RASS). The original RASS used the term “sedation” which was changed to “drowsy”.